Causes of Hypoglycemia: Why Low Blood Sugar Happens and What It Can Mean
Hypoglycemia means blood sugar that has dropped too low to safely support normal body function. Many people associate it only with diabetes, but the topic is broader than that. Low blood sugar can happen because of insulin or other glucose-lowering medicines, but it can also be linked to skipped meals, heavy alcohol use, intense exercise, certain illnesses, hormone problems, and, in rare cases, tumors or metabolic disorders.
This matters in real life because glucose is one of the body’s main fuel sources, especially for the brain. When blood sugar falls, a person may feel shaky, sweaty, hungry, anxious, dizzy, or mentally foggy. If it drops further, confusion, seizures, or loss of consciousness can happen. That is why understanding the causes of hypoglycemia is not just a medical detail. It affects driving, exercise, work, sleep, medication safety, and daily routines.
This guide explains what hypoglycemia is, the main types and patterns, the most common and less common causes, typical symptoms, risk factors, how clinicians evaluate it, and how to live more safely if you are prone to episodes. It is educational content, not a personal diagnosis. Severe symptoms, fainting, seizures, repeated episodes, or suspected medication-related low blood sugar deserve prompt medical care.
Understanding Hypoglycemia
Hypoglycemia is the medical term for low blood glucose. In many diabetes care settings, a blood sugar below 70 mg/dL is treated as an important low that deserves attention, even though symptoms and severity vary from person to person. Some people start to feel warning signs around that level, while others may not notice symptoms until the number is lower.
To understand the causes of hypoglycemia, it helps to know how the body normally keeps blood sugar in a healthy range. After you eat, carbohydrates are broken down into glucose and absorbed into the bloodstream. Insulin helps move that glucose into cells for energy and storage. Between meals, during sleep, or during exercise, the body keeps blood sugar stable by releasing stored glucose from the liver and by making new glucose when needed. Hormones such as glucagon, cortisol, growth hormone, and epinephrine also help prevent blood sugar from falling too far.
Hypoglycemia happens when that balance fails. Sometimes the body has too much insulin on board. Sometimes not enough food has been eaten for the situation. Sometimes the liver cannot release glucose effectively, or a person has been more physically active than usual without adjusting meals or medication. In other cases, another illness changes how the body handles glucose.
A useful way to think about hypoglycemia is this: low blood sugar is not one single disease. It is a sign that something in the body’s fuel-management system is off. For some people, the explanation is straightforward, such as taking insulin and then delaying lunch. For others, especially people without diabetes, repeated episodes may need a more careful workup.
Types Of Hypoglycemia
There are several ways to classify hypoglycemia, and each one helps explain the likely cause.
Diabetic hypoglycemia
This is the most common form. It happens in people with diabetes, especially those using insulin, sulfonylureas, or meglitinides. The usual pattern is that medicine lowers blood sugar more than expected because the meal was smaller than usual, delayed, missed, or followed by more activity than planned.
Non-diabetic hypoglycemia
This is less common and may be harder to recognize. It can occur with certain illnesses, hormone deficiencies, liver disease, kidney disease, after some types of bariatric surgery, from certain medicines, or because of rare conditions such as insulinoma.
Fasting hypoglycemia
This tends to happen when a person has not eaten for several hours or overnight. It may point toward medication effects, alcohol-related problems, serious illness, liver disease, hormone problems, or rare tumors that affect insulin levels.
Reactive hypoglycemia
Also called postprandial hypoglycemia, this happens after eating, usually within about four hours of a meal. It may occur after meals high in refined carbohydrates, after certain stomach surgeries, or in people with patterns of insulin release that overshoot what the body needs.
Mild, clinically significant, and severe hypoglycemia
Another practical way to sort episodes is by severity. Some lows cause warning symptoms but the person can self-treat. More serious lows may bring marked confusion or inability to function well. Severe hypoglycemia means the person needs help from someone else, may be unable to eat or drink safely, and may require glucagon or emergency care.
Causes Of Hypoglycemia
The phrase “causes of hypoglycemia” may sound repetitive, but the key question is simple: what actually makes blood sugar drop too low?
1. Diabetes medications
For people with diabetes, the most common cause is taking insulin or certain glucose-lowering drugs that continue working even when food intake, timing, or activity changes. A person may take their usual dose, then eat less than expected, eat later than planned, vomit, or exercise harder than usual. The medication keeps pushing sugar down, but the body does not get enough incoming fuel to match it.
Real-life example: someone takes rapid-acting insulin before dinner, then gets delayed in traffic and does not eat for 90 minutes. Another person takes a sulfonylurea in the morning, eats a small breakfast, skips lunch during a busy workday, and develops shakiness and confusion mid-afternoon. Both situations can trigger a low.
2. Missing meals or eating too little
Food gives the body incoming glucose. When meals are skipped, delayed, or unusually small, blood sugar may fall, especially in people taking diabetes medication. Even without diabetes, people who go long stretches without eating, combine fasting with alcohol, or have poor nutritional intake may feel symptomatic lows or near-lows.
This is why “healthy eating” is not just about calories or avoiding sugar. Meal timing matters too. A person may be eating “clean” but still run into trouble if breakfast is coffee only, lunch is late, and the afternoon includes a hard workout.
3. More physical activity than usual
Exercise helps muscles use glucose more efficiently. That is a major health benefit, but it can also lower blood sugar during activity and for hours afterward, particularly in people using insulin or insulin-stimulating drugs. Long walks, gym sessions, housework, yard work, sports, or physically demanding jobs can all matter.
A common mistake is planning for exercise based on “formal workouts” only. In reality, extra movement throughout the day counts too. A vacation with more walking, a warehouse shift, or carrying and climbing more than usual may change glucose needs.
4. Alcohol, especially without food
Alcohol is a well-known but often underestimated cause of hypoglycemia. One reason is that the liver helps protect blood sugar between meals by releasing stored glucose and making new glucose. Alcohol can interfere with that process. The risk is higher if a person drinks on an empty stomach, drinks heavily, or combines alcohol with insulin or certain diabetes medicines.
This helps explain why some people do not feel low right away. The episode may occur hours later, including overnight. A person may think they are simply tired from drinking, when in fact blood sugar has fallen dangerously low.
5. Reactive hypoglycemia after meals
Some people notice symptoms a few hours after eating, especially after a meal high in refined carbohydrates or sugary foods. In some cases, the body releases more insulin than needed after the meal, which then pushes blood sugar down. This pattern is sometimes called reactive or postprandial hypoglycemia. It can also happen after certain stomach surgeries, when food moves rapidly into the intestine and triggers sharp swings in glucose and insulin.
This does not mean carbohydrates are “bad.” It means the balance, pace, and composition of the meal matter. A breakfast of sweet pastry and juice may cause a faster rise and fall than a breakfast that combines oats, Greek yogurt, nuts, and fruit.
6. Illness affecting the liver, kidneys, or other major systems
The liver and kidneys both play roles in glucose control. Serious liver disease may reduce stored glucose and impair glucose production. Kidney disease can affect how the body clears insulin and certain medicines, which may increase the chance of lows. Severe infection or critical illness can also disrupt normal glucose regulation.
In practical terms, this means a medication dose that used to be safe may become too strong if kidney function worsens or appetite drops during illness. That is one reason sick-day plans are so important for people with diabetes.
7. Hormone deficiencies
Hormones help defend the body from low blood sugar. Problems involving cortisol, growth hormone, glucagon, or adrenal function can make it harder to maintain normal glucose, especially during fasting or illness. These are not the most common explanations, but they are medically important when a person has unexplained recurrent episodes.
8. Rare insulin-producing tumors or other uncommon conditions
Insulinoma is a rare pancreatic tumor that makes insulin even when the body does not need it. This can lead to repeated episodes of low blood sugar, often during fasting, overnight, or between meals. Because it is uncommon, it is not the first explanation doctors consider, but it becomes part of the workup when symptoms are recurrent and unexplained.
Rare inherited metabolic conditions and glycogen storage diseases can also contribute to hypoglycemia, especially in children, though some forms are diagnosed later.
9. Certain medicines besides diabetes drugs
Although diabetes medicines are the biggest medication-related cause, some non-diabetes drugs can also contribute in certain people. This may include some antibiotics and other medicines depending on the person’s health status, kidney function, nutrition, and other medications.
10. Weight loss surgery and altered digestion
After some bariatric procedures, food can move through the stomach more quickly than before. This may create rapid changes in blood sugar and insulin release after meals, leading to post-meal lows in some people.
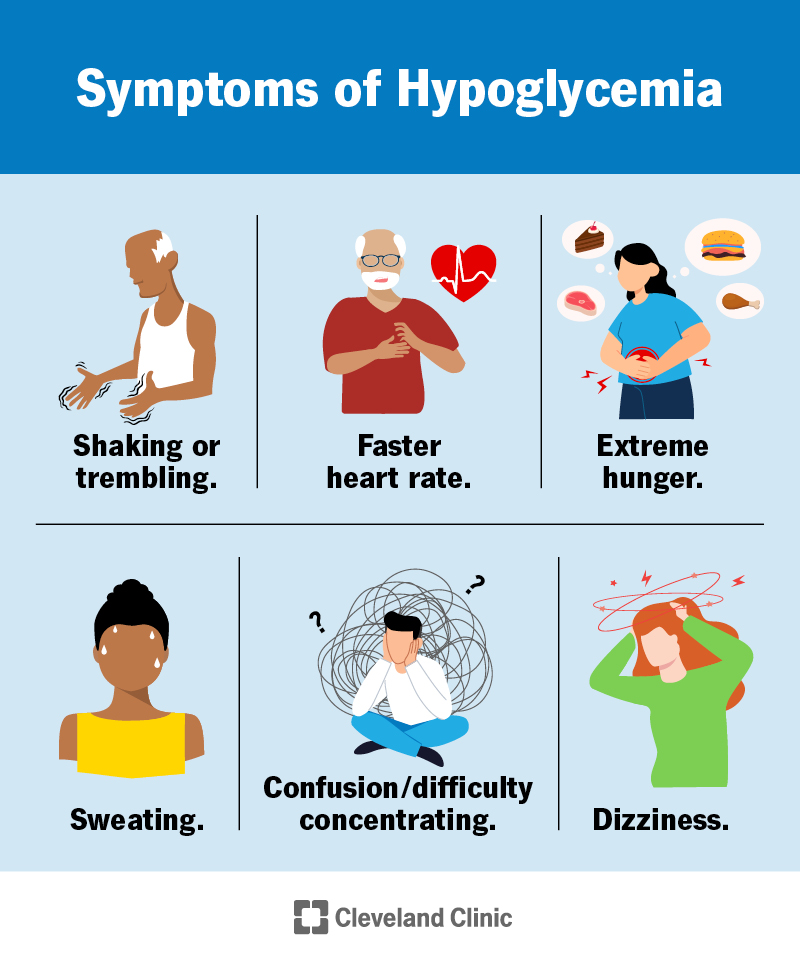
Symptoms Of Hypoglycemia
The symptoms of hypoglycemia come from two main processes. First, the body releases stress hormones to try to raise blood sugar, which can trigger shakiness, sweating, fast heartbeat, and anxiety. Second, the brain begins to run short on glucose, which can cause trouble thinking clearly, visual changes, clumsiness, confusion, and eventually seizures or loss of consciousness.
Common early symptoms include:
- Shaking or trembling
- Sweating
- Fast heartbeat
- Hunger
- Dizziness or lightheadedness
- Nervousness or anxiety
- Irritability
- Headache
- Weakness or fatigue
As blood sugar drops further, symptoms may include:
- Confusion
- Trouble concentrating
- Blurred vision or double vision
- Slurred speech
- Poor coordination
- Behavioral changes
- Severe drowsiness
- Seizure
- Loss of consciousness
Not everyone feels hypoglycemia the same way. Some people mainly feel hunger and sweating. Others feel anxious or suddenly “off.” Some wake from sleep drenched in sweat or with nightmares and morning headaches. People who have had diabetes for a long time may develop hypoglycemia unawareness, meaning their early warning signs become weaker or disappear. That makes severe episodes more dangerous because there is less time to react.
In real life, symptoms can be mistaken for other things. A person may think they are having a panic attack, are overly tired, or are simply “hangry.” That is one reason pattern tracking matters. If symptoms repeatedly improve after glucose, food, or adjusting medication timing, that is important information to bring to a clinician.
Risk Factors
Some people are more likely to experience hypoglycemia than others.
Diabetes treatment with insulin or insulin-stimulating drugs
This is the biggest risk factor. The more tightly medication is matched to food and activity, the more any disruption in routine can matter.
Irregular eating patterns
Skipping breakfast, long fasting windows, very low calorie diets, nausea, poor appetite, or unpredictable work schedules can increase risk.
Increased or unplanned physical activity
Exercise, manual labor, travel days, active vacations, and intense weekend sports can all change glucose needs.
Alcohol use
The risk rises when alcohol is used without food, in larger amounts, or with insulin or sulfonylureas.
Kidney or liver disease
These conditions can change glucose regulation and medication handling.
Older age
Older adults may be more vulnerable because of medication complexity, reduced appetite, kidney changes, memory problems, or difficulty recognizing symptoms early. This is an inference based on established clinical risk patterns tied to medication safety and organ function.
Previous severe hypoglycemia or hypoglycemia unawareness
A prior serious episode is a warning sign that future episodes may also become severe if nothing changes.
Diagnosis Process
The evaluation depends on whether the person has diabetes, how often episodes happen, whether symptoms match measured low glucose, and whether the episodes occur fasting or after meals.
For a person with diabetes, clinicians often start with practical questions:
- What medications are you taking?
- When do the lows happen?
- What did you eat before the episode?
- Was exercise, alcohol, illness, or vomiting involved?
- How low was the reading?
- Did you need help from someone else?
Blood sugar logs and continuous glucose monitor data can be very helpful. They can show whether lows cluster overnight, after exercise, before lunch, or after certain meals. That makes it easier to see patterns instead of guessing.
For people without diabetes, the workup may be more detailed. Clinicians often look for a pattern sometimes described as symptoms that occur with low measured blood sugar and improve when glucose is corrected. Depending on the situation, testing may include lab work, medication review, liver and kidney assessment, hormone testing, or supervised fasting evaluation. In some cases, an extended fast in a medical setting is used to safely provoke and study fasting hypoglycemia.
When episodes happen after meals, the evaluation may focus more on meal composition, timing, digestive surgery history, and whether symptoms truly match low glucose. Not every “sugar crash” is true hypoglycemia, which is why measurement matters.
Living With Hypoglycemia
Living with a tendency toward low blood sugar often means learning patterns rather than living in fear. Many people become more confident once they understand their triggers: a missed snack before a long commute, an evening workout without adjusting dinner, wine without food, or taking medication and then unexpectedly eating late.
Day to day, the goal is not perfection. It is predictability. Many people do better when they keep meals more consistent, carry a quick glucose source, avoid “guessing” about symptoms, and review episodes instead of brushing them off. Someone who gets shaky every afternoon at 4 p.m. does not just need willpower. They need to figure out whether lunch is too light, medication is mistimed, or physical activity is higher than expected.
Sleep can also be affected. Overnight lows may cause restless sleep, sweating, vivid dreams, morning headache, or waking up feeling drained. People who have frequent nighttime episodes may need medication adjustments, bedtime snack changes, or closer monitoring, especially if they live alone or do not wake to symptoms.
Emotionally, hypoglycemia can be draining. Some people start overeating “just in case,” which can lead to rebound high blood sugar and frustration. Others become afraid to exercise or keep their glucose higher than recommended because lows feel so unpleasant. These reactions are understandable, but they often mean the prevention plan needs improvement, not that the person has failed.
Prevention Strategies
Prevention depends on the cause, but several strategies help many people.
Know your main trigger pattern
Is the problem happening because of missed meals, too much medication, exercise, alcohol, or post-meal swings? Prevention gets easier when the pattern is clear.
Do not skip meals if your treatment plan makes that risky
If you use insulin or medicines that can lower glucose independently, meal timing matters. Regular intake is often safer than “winging it.”
Pair carbohydrates with protein, fat, or fiber when appropriate
For people prone to post-meal crashes, meals built around balanced composition may support steadier glucose than meals centered on sugary drinks or refined carbohydrates alone.
Plan for exercise
Check glucose if recommended for your situation, bring fast carbohydrate, and discuss medication adjustments if exercise often triggers lows.
Be cautious with alcohol
Avoid drinking on an empty stomach, and talk with a clinician about what is safe for your medications and health status.
Carry treatment
Quick sugar sources such as glucose tablets, juice, or hard candy can help treat early hypoglycemia quickly. People at risk for severe episodes may also need glucagon available and should make sure family, friends, coworkers, or roommates know how to use it.
Use monitoring tools wisely
For some people, frequent finger-stick checks or continuous glucose monitoring can reduce surprises and reveal patterns.
Review recurring lows with a clinician
Repeated episodes are not something to simply “push through.” Treatment plans often need adjustment after recurrent hypoglycemia.
Practical Examples
A simple daily checklist
- Eat meals on a predictable schedule if you are prone to lows.
- Keep a rapid glucose source in your bag, desk, car, or gym pouch.
- Do not drink alcohol without eating.
- Pay attention on unusually active days.
- Record when lows happen and what was going on beforehand.
- Review repeated episodes with your healthcare professional.
Sample balanced meal ideas for people prone to post-meal crashes
- Oatmeal with Greek yogurt, berries, and nuts
- Whole-grain toast with eggs and avocado
- Chicken, brown rice, and vegetables
- Apple slices with peanut butter
- Plain yogurt with seeds and fruit
These are not special “hypoglycemia foods.” They are examples of meals and snacks that may digest more steadily than highly refined, sugary choices eaten alone.
A beginner routine for someone with diabetes who gets afternoon lows
- Eat breakfast and lunch at more consistent times.
- Keep lunch balanced rather than carb-heavy and protein-poor.
- Track medication timing.
- Notice whether work, walking, or workouts increase before the low.
- Carry glucose tablets.
- Review the pattern with your clinician instead of just adding extra random snacks every day.
Common mistakes
- Taking medication and then delaying the meal
- Treating every shaky feeling as hunger without checking patterns
- Overtreating lows with large amounts of sweets, then rebounding high
- Ignoring nighttime symptoms
- Assuming exercise only matters during the workout itself
- Drinking alcohol without food
- Having repeated lows and never telling a clinician
When urgent care is needed
Get emergency help if low blood sugar causes seizure, unconsciousness, inability to swallow safely, or severe confusion, or if symptoms do not improve as expected. Severe hypoglycemia can be dangerous and may require glucagon or emergency medical treatment.
Conclusion
The causes of hypoglycemia range from common daily issues to uncommon medical disorders. In people with diabetes, the usual causes are medication, missed or delayed meals, exercise, and alcohol. In people without diabetes, recurring episodes can sometimes point to digestive changes after surgery, major illness, hormone problems, medication effects, or, rarely, insulin-producing tumors.
The most practical takeaway is that low blood sugar is often pattern-based. It usually becomes easier to manage when you stop viewing it as random bad luck and start asking better questions: What happened before it? Was food delayed? Was activity higher? Was alcohol involved? Did it happen fasting or after a meal?
If you have repeated episodes, nighttime lows, symptoms without a clear cause, or any severe event, the next step should be medical review. Safe management depends on the individual, the underlying cause, and the treatment plan.