ALS Causes: What Researchers Know About Why ALS Happens, Genetic Links, and Risk Factors

If you are searching for ALS causes, you are probably asking a very human question: why does this disease happen at all? That question matters not only to people who are worried about symptoms, but also to families trying to understand risk, caregivers planning ahead, and readers who want a clear, grounded explanation without medical jargon.
ALS, or amyotrophic lateral sclerosis, is a progressive disease that affects the nerve cells that control voluntary muscles. Over time, it can interfere with walking, using the hands, speaking, swallowing, and breathing. In most cases, the exact cause is still unknown. A smaller share of cases runs in families and is linked to inherited gene changes.
This article explains what doctors and researchers currently know about ALS causes, what is still uncertain, which symptoms and risk factors matter in real life, how diagnosis usually happens, and what daily management often looks like after diagnosis. This is educational content, not a diagnosis. If you or someone you love has progressive weakness, speech changes, trouble swallowing, or unexplained breathing symptoms, it is important to speak with a qualified healthcare professional promptly.
Understanding als causes
ALS is a motor neuron disease. That means it damages the nerve cells responsible for sending movement signals from the brain and spinal cord to the muscles. These nerve cells include upper motor neurons, which carry signals from the brain downward, and lower motor neurons, which carry signals from the spinal cord to muscles throughout the body. When these neurons deteriorate and die, the muscles stop receiving clear instructions. As a result, muscles become weak, may twitch, and eventually waste away.
This helps explain why ALS is so disruptive in everyday life. It does not start as a vague “nerve problem.” It starts as a communication failure between the nervous system and the muscles you use to do ordinary things: buttoning a shirt, lifting a cup, climbing stairs, speaking clearly, chewing food, and taking a deep breath. The damage tends to worsen over time because more motor neurons are affected as the disease progresses.
 One detail many people find surprising is that ALS usually does not affect the senses in the way other neurological conditions can. Taste, smell, touch, and hearing are usually preserved. Bladder function also is not usually affected in the typical course of ALS. That can be important because it helps explain why a person may remain mentally aware of physical decline, which can make the illness emotionally and practically demanding.
One detail many people find surprising is that ALS usually does not affect the senses in the way other neurological conditions can. Taste, smell, touch, and hearing are usually preserved. Bladder function also is not usually affected in the typical course of ALS. That can be important because it helps explain why a person may remain mentally aware of physical decline, which can make the illness emotionally and practically demanding.
When people ask about “ALS causes,” they often imagine there must be one trigger. In reality, the current medical view is more complex. The leading idea is that ALS often reflects an interaction between genetic susceptibility and other biological or environmental influences. In some people, inherited mutations play a major role. In many others, no single cause can be identified.
Types Of als causes
Sporadic ALS
The most common form is sporadic ALS, which makes up about 90% of cases. “Sporadic” means it appears without a clear family history and without one obvious known trigger. This is the form most people are referring to when they talk about ALS in general conversation.
Sporadic does not mean “simple.” It means the cause is not fully explained. A person may never know exactly why the disease developed. Researchers continue studying whether a mix of subtle genetic changes, age-related biological stress, and outside exposures may combine over time in some people.
Familial ALS
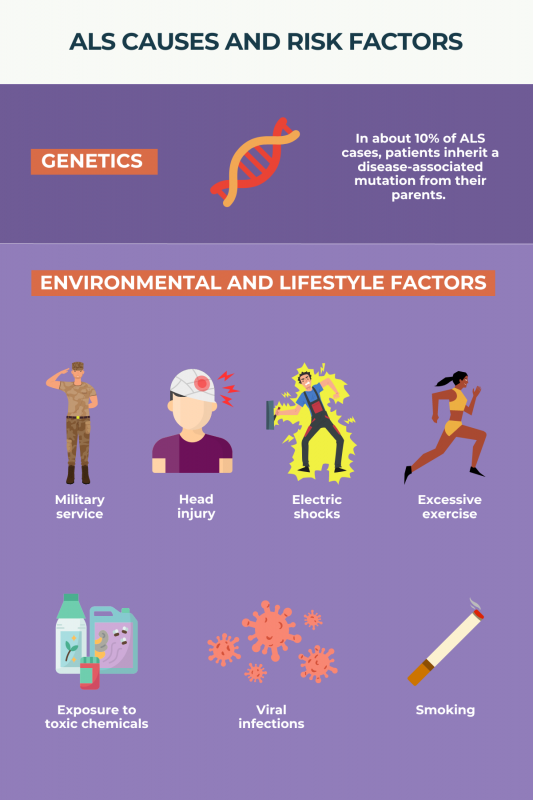
The less common form is familial ALS, which usually accounts for about 5% to 10% of cases. This form runs in families and is linked to inherited gene changes passed from parent to child. If a parent carries a disease-causing mutation for hereditary ALS, children may have a significant chance of inheriting that mutation, depending on the specific genetic pattern involved.
Several genes are strongly associated with familial ALS. Commonly discussed examples include C9orf72, SOD1, TARDBP, and FUS. These genes do not all behave in exactly the same way, and they may influence how the disease begins, how fast it progresses, or whether symptoms overlap with other neurological conditions such as frontotemporal dementia.
Limb-onset and bulbar-onset patterns
Doctors also describe ALS by how it starts, even though these are not “causes” in the strict sense. Some people have limb-onset ALS, where weakness begins in a hand, arm, foot, or leg. Others have bulbar-onset ALS, where early problems involve speech or swallowing. This distinction matters in real life because the first symptoms shape how quickly people notice the problem and what kind of help they may need first.
For example, limb-onset disease may first look like clumsiness, frequent tripping, foot drop, or an increasingly weak grip. Bulbar-onset disease may first show up as slurred speech, choking on liquids, taking much longer to finish meals, or people repeatedly asking the person to repeat themselves.
Causes Of als causes
The short answer: most ALS cases do not have one proven cause
The most honest answer to “what causes ALS?” is this: most cases do not have one confirmed, single cause. Major medical organizations state that the exact cause remains unknown for most people. That is especially true for sporadic ALS.
That uncertainty can be frustrating, but it also matters for accuracy. ALS is not currently understood as a disease with one universal trigger such as one virus, one food pattern, or one lifestyle choice. Anyone who promises a single neat answer is oversimplifying what the evidence actually shows.
Genetics may be the clearest established cause in some people
For familial ALS, inherited gene changes are the clearest known cause. Researchers have identified multiple genes involved, with C9orf72, SOD1, TARDBP, and FUS among the most established. Some of these gene changes can also appear in a small percentage of people who seem to have sporadic ALS, which suggests genetics may matter even when there is no obvious family history.
This does not mean every person with ALS should assume their children will get the disease. It means that when there is a strong family history, or when a neurologist suspects inherited ALS, genetic counseling and targeted testing may become part of the evaluation. That conversation can help families understand what is known, what remains uncertain, and what the results may or may not mean for relatives.
Environment may contribute, but the evidence is mixed
Environmental factors have been studied for years, but the evidence is more cautious than many headlines suggest. Some studies have suggested possible links with smoking, certain heavy metals, other workplace or home toxic exposures, and military service. At the same time, public health sources emphasize that no single environmental cause has been consistently confirmed for most ALS cases.
This distinction is important. A factor can be associated with increased risk without being proven to directly cause the disease in any one person. For example, if a veteran develops ALS, it does not automatically mean military service caused it. It means researchers have observed a pattern worth studying further. The same caution applies to smoking and toxin exposure.
The likely real-world model is “multiple hits,” not one event
A practical way to understand current thinking is the “multiple-hit” model. In simple terms, a person may have a certain genetic vulnerability, age-related changes in nerve cells, and perhaps one or more environmental influences. Over time, those layers may combine in a way that pushes motor neurons past the point where they can keep functioning normally.
That idea also explains why ALS can look so different from one person to another. Two people may both have ALS, yet one may start with speech problems in their 50s while another begins with leg weakness much later. Their disease may share a final pathway, but not necessarily the same exact sequence of causes.
Symptoms Of als causes
ALS symptoms vary depending on which motor neurons are affected first and how the disease spreads. A common early pattern is muscle weakness that gradually worsens. People may notice trouble walking, frequent tripping, weakness in the feet or ankles, hand clumsiness, slurred speech, difficulty swallowing, muscle cramps, or visible twitching in the arms, shoulders, hands, feet, or tongue.
In real life, these symptoms often start subtly. Someone may realize they keep dropping keys. A formerly steady walker may start catching one foot on steps. A person who talks all day at work may sound unusually tired or slightly slurred by evening. Another person may take much longer to finish meals because swallowing feels less automatic.
As ALS advances, weakness tends to spread. This can affect chewing, speaking, swallowing, standing, walking, and breathing. Weight loss may follow when eating becomes difficult. Breathing problems may start quietly, sometimes showing up first as waking up tired, feeling short of breath when lying flat, or needing more pauses while speaking.
Some people also experience pseudobulbar affect, which means episodes of laughing, crying, or yawning that happen at inappropriate times or feel out of proportion to the situation. Thinking or behavioral changes can occur in some cases, and a subset of people with ALS develop problems related to frontotemporal dementia.
A key point for readers: ALS often causes weakness without the kind of numbness or loss of sensation people may expect from other nerve disorders. That is one reason ALS can be confusing early on. The person may feel physically weaker while still being able to feel touch, temperature, and pain normally.
 Risk Factors
Risk Factors
Age
Age is one of the clearest risk factors. ALS is most often diagnosed in later adulthood, with many cases appearing between about 55 and 75, though some sources describe a broader common range extending into the mid-80s. It can happen earlier or later, but the overall risk rises with age.
Genetics and family history
A known family history of ALS is one of the strongest risk clues because hereditary ALS is driven by inherited gene changes. When several relatives on one side of the family have ALS, or ALS plus frontotemporal dementia, that pattern may prompt genetic evaluation.
Sex
ALS has historically been reported as slightly more common in men than women, especially before age 65. That gap appears to narrow later in life. This is a population-level observation, not a rule for individuals, and it does not mean women are protected.
Smoking
Smoking is one of the more consistent modifiable risk factors discussed in clinical summaries. It does not mean smokers will develop ALS, and many people with ALS never smoked. Still, the evidence is strong enough that smoking is often listed among established or likely environmental risk factors.
Military service and possible exposure patterns
Studies indicate that people who have served in the military may have a higher risk of ALS. Researchers do not know whether that pattern reflects chemical exposure, metals, traumatic injury, intense exertion, or some combination of factors. This is an area of active study, not a settled explanation.
Toxins and occupational exposures
Possible links have also been studied for lead, mercury, solvents, pesticides, and other occupational or environmental toxicants. The practical takeaway is careful but simple: some exposures may matter, but no single toxin has been consistently proven as the main cause of ALS in the general population.
Diagnosis Process
ALS can be difficult to diagnose early because its symptoms overlap with many other neurological and muscle disorders. There is no single test that simply confirms ALS in every case. Diagnosis usually depends on a neurologic exam, the pattern of symptoms over time, and testing that helps rule out other possible explanations.
A typical evaluation often includes:
- A detailed medical history
- A neurological exam
- Electromyography (EMG)
- Nerve conduction studies
- MRI of the brain or spine
- Blood and urine testing
- Sometimes a lumbar puncture
- In selected cases, a muscle biopsy or nerve biopsy
EMG is especially important because it helps doctors assess electrical activity in muscles and look for patterns of nerve-related damage. MRI is often used not because it “shows ALS” directly in every case, but because it helps exclude problems such as spinal cord compression, tumors, or other structural conditions that can mimic ALS symptoms.
In practical terms, that means many people do not leave the very first appointment with a final answer. The process may involve repeat visits and repeated testing, especially when symptoms are mild or unusual at the beginning. This delay can be emotionally hard, but it reflects the reality that clinicians need to be careful before confirming a serious diagnosis like ALS.
Living With als causes
Living with ALS is about much more than knowing what may have caused it. Once the disease is present, the day-to-day questions become urgent: How will I eat? Work? Communicate? Move safely? Sleep? Breathe? The best care usually comes from a multidisciplinary team that may include a neurologist, respiratory therapist, speech therapist, physical therapist, occupational therapist, dietitian, mental health support, and palliative care support.
Treatment cannot reverse the nerve damage already done, but it may help slow progression and improve comfort and function. Current medical options commonly include riluzole, which may extend survival modestly, edaravone, which may slow decline in daily functioning for some people, and tofersen for people with SOD1-associated ALS. Symptom-focused treatment may also be needed for cramps, spasticity, sleep problems, excess saliva, pain, constipation, mood symptoms, and episodes of uncontrolled laughing or crying.
Therapy is often one of the most practical parts of care. Physical therapy may help with safe movement and energy conservation. Occupational therapy can help with braces, wheelchairs, bathroom modifications, dressing tools, and ways to reduce fatigue during daily tasks. Speech therapy may help preserve communication and support safer swallowing for as long as possible.
Nutrition becomes a central issue sooner than many families expect. If swallowing becomes difficult, a person may eat less, lose weight, get dehydrated, or accidentally inhale food or liquids into the lungs. A dietitian can help adapt meals, and in some cases a feeding tube may reduce choking risk and help maintain nutrition and hydration.
Breathing support also becomes critical as ALS progresses. Noninvasive ventilation through a mask may improve comfort, especially at night, and later some people consider tracheostomy-based ventilation. Shortness of breath, repeated chest infections, weak cough, trouble clearing the throat, or inability to lie flat are warning signs that need prompt medical attention. Emergency care is needed for significant breathing difficulty.
The emotional side is just as real as the physical side. Depression, anxiety, grief, frustration, and caregiver burnout are all common concerns in serious progressive illness. Asking for counseling, support groups, social work help, or palliative care is not “giving up.” It is part of good care.
Life expectancy varies widely. Public health and specialty sources note that many people live roughly 2 to 5 years after symptoms begin or about 3 to 5 years after diagnosis, yet some live much longer, including 10 years or more. The exact course depends on age, symptom pattern, breathing involvement, swallowing issues, and likely biology that is still not fully understood.
Prevention Strategies
There is currently no proven way to prevent ALS. That is one of the hardest truths around this topic, and it is worth stating clearly. Even people who do everything “right” can still develop sporadic ALS, because the disease usually does not come from one obvious controllable cause.
That said, “no proven prevention” does not mean “nothing sensible matters.” Practical risk-reduction steps may still be reasonable, especially when they align with broader health goals:
- Do not smoke, or seek support to quit
- Use appropriate protective equipment if you work around chemicals, dusts, solvents, metals, or pesticides
- Take persistent weakness, speech changes, swallowing problems, or unexplained muscle wasting seriously
- Ask about genetic counseling if there is a strong family history of ALS or related dementia
- Maintain regular medical care so concerning symptoms are not brushed off or delayed
A practical way to think about prevention is this: you may not be able to eliminate risk, but you can still reduce avoidable exposures, improve early recognition, and make sure any suspicious symptoms are evaluated before dangerous complications develop. That may not stop ALS from existing, but it can support safer, faster care.
Practical Examples
Example 1: When “clumsiness” is no longer normal
A 58-year-old person notices they keep tripping on the same foot and can no longer lift grocery bags the way they used to. At first, they assume it is aging, overwork, or a back problem. After a few months, the weakness is clearly getting worse rather than better.
The practical move here is not panic, but prompt evaluation. Progressive weakness, repeated falls, obvious muscle wasting, or slurred speech should not be watched for months without medical input. A primary care clinician may refer the person to neurology for further testing.
Example 2: Eating becomes stressful
A person with bulbar symptoms starts coughing during meals, avoiding dry foods, and taking an hour to finish dinner. Family members notice weight loss and more throat clearing.
In this situation, practical support may include a swallowing evaluation, speech therapy, softer and easier-to-swallow foods, higher-calorie meals in smaller portions, and discussion of whether a feeding tube may become helpful later. Waiting too long can increase the risk of dehydration, malnutrition, and aspiration pneumonia.
Example 3: A better daily routine after diagnosis
A realistic starter routine for someone living with ALS may look like this:
- Morning: take medications, do gentle stretching or therapist-guided movement, use adaptive tools for dressing
- Midday: eat a calorie-dense, easy-to-swallow lunch, rest before fatigue builds
- Afternoon: schedule important tasks when energy is best, use mobility aids instead of pushing through exhaustion
- Evening: prepare communication tools for the next day, reduce fall hazards, use breathing support if prescribed at night
The goal is not to “stay strong by pushing harder.” The goal is to conserve energy, maintain safety, and protect breathing and nutrition.
Example 4: A simple home checklist
A practical home checklist may include:
- Remove loose rugs and trip hazards
- Keep frequently used items at waist level
- Add grab bars in the bathroom
- Use chairs with arms for easier standing
- Keep a written medication list visible
- Track weight, swallowing changes, and breathing symptoms
- Tell the care team early about weak cough, choking, or lying-flat shortness of breath
Do’s and don’ts for beginners
Do:
- Seek evaluation for progressive weakness or speech/swallowing changes
- Ask specific questions about breathing, nutrition, and home safety
- Bring a family member to appointments
- Write down symptom changes between visits
- Accept adaptive devices early if they reduce falls and fatigue
Don’t:
- Assume all weakness is just aging
- Keep forcing hard-to-swallow foods
- Ignore repeated chest infections or weak cough
- Wait for “severe” symptoms before discussing ventilation or feeding support
- Try unproven cures in place of medical care
Conclusion
When people search for ALS causes, they are often hoping for certainty. Right now, the clearest answer is that most ALS cases do not have one confirmed cause, while a smaller group is linked to inherited genetic mutations. The strongest current framework is that ALS may result from a complicated interaction between genes, biology, age, and possibly environmental influences rather than one simple trigger.
What matters most in practical terms is early recognition and timely support. Progressive weakness, trouble speaking, difficulty swallowing, unexplained muscle wasting, or breathing changes deserve medical attention. Even though ALS cannot currently be cured, earlier diagnosis and multidisciplinary care may help preserve comfort, function, nutrition, communication, and safety for as long as possible.