Brain Atrophy: Causes, Symptoms, Types, Diagnosis, and What It Can Mean for Daily Life
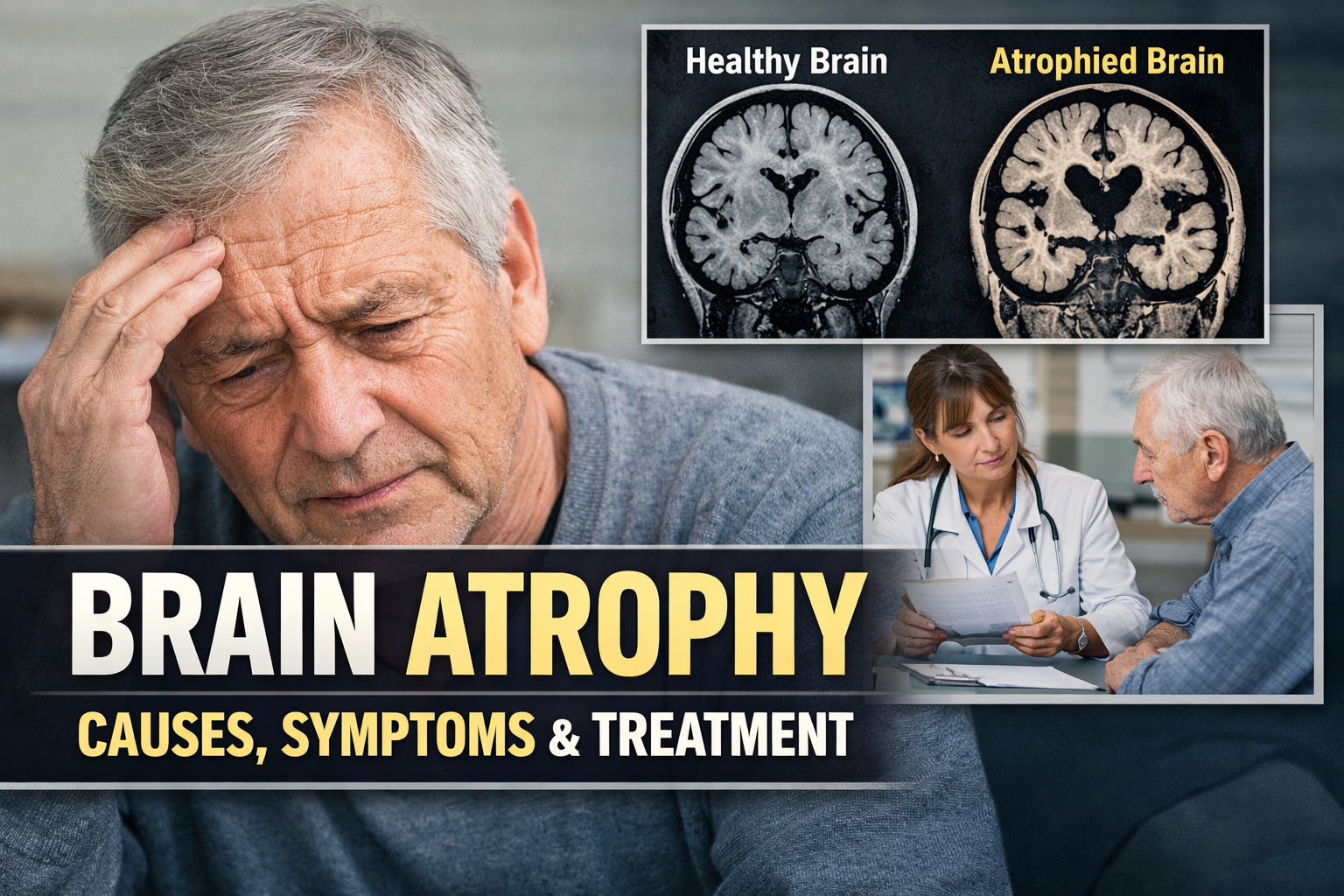
Brain atrophy, also called cerebral atrophy, means there has been a loss of brain cells and the connections between them. In simple terms, parts of the brain become smaller because neurons are damaged or lost. Some brain shrinkage can happen with normal aging, but faster or more pronounced atrophy may point to an underlying medical problem such as a neurodegenerative disease, stroke-related damage, infection, autoimmune disease, or traumatic brain injury.
What makes brain atrophy important is not just the scan result itself, but why it is happening and whether it is affecting memory, thinking, movement, language, or behavior. A person can have mild structural changes on imaging with few obvious symptoms, while someone else may have atrophy that clearly affects daily function. That is why brain atrophy is not a diagnosis by itself. It is a finding that needs to be interpreted in clinical context.
This guide explains what brain atrophy is, the main types, common causes, symptoms to watch for, how doctors evaluate it, and what steps may help support brain health.
What Is Brain Atrophy?
Brain atrophy is the loss of neurons and the connections between neurons, which leads to a reduction in brain volume. The changes may involve one region or many areas of the brain. Depending on the location, a person may develop memory problems, trouble with speech, personality changes, coordination issues, or other neurologic symptoms.
It is important to separate normal age-related brain changes from more concerning atrophy. Aging can affect brain structure over time, but pathological atrophy tends to be faster, more selective, or linked with symptoms that interfere with everyday life. In conditions such as Alzheimer’s disease and other dementias, brain shrinkage reflects disease-related injury rather than routine aging alone.
Types of Brain Atrophy
Focal brain atrophy
Focal atrophy means shrinkage is centered in a specific area of the brain. This may happen after a stroke, localized trauma, infection, or a disease that targets a particular region. Symptoms usually reflect the job of the affected area. For example, damage in language areas may cause word-finding difficulty, while damage in balance-related regions may affect coordination.
Generalized brain atrophy
Generalized atrophy means tissue loss is spread more broadly across the brain. This pattern may be seen in some neurodegenerative diseases, chronic vascular injury, long-term alcohol-related brain injury, or other systemic conditions that affect the brain more diffusely. Widespread atrophy is more likely to be associated with broad changes in cognition and daily function.
Cortical vs. subcortical atrophy
Cortical atrophy affects the outer layer of the brain, the cerebral cortex, which is involved in language, memory, judgment, sensory processing, and voluntary movement. Subcortical atrophy affects deeper structures that help regulate movement, attention, alertness, and communication between brain regions. Some disorders mainly affect one pattern, while others involve both.
Region-specific atrophy
Sometimes doctors describe atrophy by the area involved, such as hippocampal atrophy, frontal lobe atrophy, temporal lobe atrophy, or cerebellar atrophy. Hippocampal atrophy is often discussed in memory disorders. Frontal and temporal patterns may be linked with personality, language, or behavior changes. Cerebellar atrophy is more closely tied to balance, coordination, and speech problems.
Common Causes of Brain Atrophy
1. Normal aging
The brain changes with age, and some shrinkage can occur over time even in otherwise healthy adults. But age-related change alone should not be used to explain significant cognitive decline without proper evaluation. Symptoms that are getting worse, or that interfere with daily life, deserve medical attention.
2. Alzheimer’s disease and other neurodegenerative diseases
Alzheimer’s disease is one of the best-known causes of progressive brain atrophy and is associated with loss of memory, thinking skills, and independence over time. Other neurodegenerative conditions can also lead to atrophy, including frontotemporal dementia, Parkinson’s-related cognitive decline, Huntington’s disease, multiple system atrophy, and amyotrophic lateral sclerosis in some cases. The exact pattern depends on which brain networks are being damaged.
3. Stroke and blood vessel disease
A stroke can leave behind permanent tissue loss in the area that was injured. More gradual blood vessel damage can also reduce blood flow to the brain over time, contributing to atrophy and vascular cognitive impairment. High blood pressure, diabetes, smoking, and high cholesterol all matter here because they affect the health of blood vessels that support the brain.
4. Traumatic brain injury
A major head injury can damage brain tissue directly. Repeated head trauma may also contribute to long-term degeneration and regional atrophy. In some people, these changes show up months or years after the original injuries and may be linked to problems with memory, mood, attention, or coordination.
5. Infections affecting the brain
Certain infections can injure brain tissue and later lead to atrophy. Examples include severe viral encephalitis, meningitis-related complications, HIV-associated brain injury, and rare prion diseases. The extent of lasting damage depends on the cause, severity, and how quickly treatment begins.
6. Autoimmune, inflammatory, and metabolic disorders
Conditions that involve inflammation, immune attack, or disrupted metabolism can also damage brain tissue. Multiple sclerosis is one example in which both inflammation and tissue loss can contribute to symptoms. Nutritional deficiency, alcohol-related injury, and other systemic illnesses may also play a role.
7. Genetic disorders
Some forms of brain atrophy are tied to inherited conditions. These are less common overall, but they matter especially when symptoms begin unusually early or there is a strong family history of neurologic disease.
Symptoms of Brain Atrophy
Symptoms depend on where the brain is affected and how extensive the tissue loss is.
Cognitive symptoms
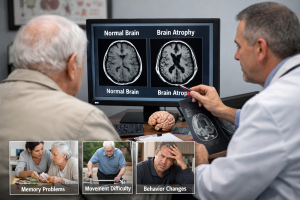
Common cognitive symptoms may include memory loss, difficulty concentrating, slower thinking, trouble planning or organizing, poor judgment, and confusion. Language problems may also occur, including difficulty finding words, following a conversation, or understanding complex information. In some disorders, the earliest changes are subtle and may look like “brain fog” or unusual forgetfulness at first.
Motor and coordination changes
If the atrophy affects movement-related networks, a person may develop clumsiness, poor balance, tremor, slowed movement, trouble walking, or loss of coordination. Cerebellar degeneration, for example, is well known for causing balance problems, speech difficulty, and coordination issues.
Behavioral and emotional changes
Some people develop personality changes, reduced motivation, depression, anxiety, irritability, emotional instability, or social withdrawal. When frontal or temporal brain regions are involved, family members may notice changes in behavior, empathy, judgment, or inhibition before memory problems become obvious.
Sensory and perception-related symptoms
Atrophy affecting visual or sensory processing areas can lead to trouble reading, judging distance, recognizing objects, or navigating familiar places. Posterior cortical atrophy, for example, may begin with visual-spatial problems rather than classic memory complaints.
When Brain Atrophy May Be Found
Brain atrophy may show up after a workup for symptoms like memory changes, confusion, movement problems, seizures, balance issues, or behavior changes. Sometimes it is seen on imaging done for another reason and becomes an incidental finding that still needs interpretation based on age, symptoms, and medical history.
How Doctors Diagnose Brain Atrophy
Brain imaging
MRI is one of the main tools used to assess brain atrophy because it gives detailed images of brain structure and can help show which regions are affected. CT can also show atrophy, but MRI is generally more informative for subtle changes and pattern recognition in cognitive disorders. Imaging can help identify enlargement of the ventricles, widening of brain grooves, and shrinkage in specific regions.
Cognitive and neurologic assessment
Doctors usually combine imaging with a neurologic exam and cognitive testing. This helps determine whether the structural change is actually linked to meaningful problems with memory, language, attention, judgment, movement, or daily function. Imaging alone does not tell the whole story.
Blood tests and other workup
Blood tests may be ordered to look for potentially treatable contributors such as thyroid disease, vitamin deficiencies, metabolic problems, or infection. In some situations, cerebrospinal fluid testing or genetic testing may be considered, depending on the clinical picture.
Can Brain Atrophy Be Reversed?
In general, lost brain tissue is not restored in the way people often hope. That said, the brain has some ability to adapt, and function can sometimes improve when the underlying cause is treated, symptoms are managed, and rehabilitation is started early. For example, treatment may aim to control inflammation, reduce vascular risk, manage neurodegenerative symptoms, support recovery after injury, or correct nutritional problems.
So while the structural shrinkage itself is usually not “reversed,” the outcome is not always hopeless. Stabilization, slowing of progression, and better day-to-day function are realistic goals in many cases.
Risk Factors That Can Increase the Chance of Brain Atrophy
Several factors linked to cognitive decline and brain injury are also relevant to atrophy risk. These include older age, family history of certain neurologic diseases, high blood pressure, diabetes, smoking, harmful alcohol use, physical inactivity, poor sleep, social isolation, depression, and exposure to head trauma. Not all risk factors are preventable, but many are modifiable.
What May Help Protect Brain Health
No single habit guarantees prevention, but research and public health guidance consistently support a brain-healthy lifestyle.
Stay physically active
Regular physical activity supports cardiovascular health and may help slow cognitive decline. Some research cited by the National Institute on Aging suggests exercise may support regions involved in memory and learning.
Control blood pressure, blood sugar, and cholesterol
Vascular health and brain health are closely connected. Managing hypertension, diabetes, and cholesterol can help lower the risk of brain injury related to poor circulation and dementia-related decline.
Do not smoke and avoid harmful alcohol use
Smoking and heavy alcohol use are associated with cognitive decline and brain injury risk. Reducing or avoiding them can benefit both brain and overall health.
Eat in a brain-supportive way
A dietary pattern built around vegetables, fruits, whole grains, legumes, nuts, fish, and healthier fats is often recommended for cardiovascular and cognitive health. While diet alone is not a treatment for brain atrophy, it supports the systems that keep the brain functioning well.
Keep your brain and social life engaged
Learning, reading, problem-solving, meaningful conversation, and social interaction may help build cognitive reserve and support healthier aging.
Protect your head and prioritize sleep
Preventing head injuries matters, especially in sports, work, and driving. Good sleep also matters because the brain relies on restorative sleep for maintenance and healthy function.
When to Seek Medical Attention
A person should seek medical evaluation if they have:
- worsening memory loss
- new confusion
- trouble speaking or understanding speech
- sudden balance or walking problems
- personality or behavior changes
- difficulty managing medications, bills, or daily tasks
- new neurologic symptoms after a head injury
- any sudden neurologic change that could suggest a stroke, such as facial droop, weakness, severe confusion, or trouble speaking
Progressive symptoms should not be dismissed as “just aging” without a proper workup. Early evaluation can help identify treatable causes and clarify what kind of support or follow-up is needed.
Living With Brain Atrophy
Living with brain atrophy often means focusing on function, safety, and support, not just imaging findings. Useful strategies may include medication review, physical therapy, occupational therapy, speech therapy, home safety changes, calendars and reminder tools, caregiver education, and regular follow-up with a neurologist or other clinician managing the underlying condition.
People and families often do better when they plan early, especially if symptoms are progressive. That can include discussing driving safety, medication routines, finances, daily supervision needs, and legal planning while the person can still participate fully in decisions. This can preserve autonomy and reduce stress later on.
FAQ
Is brain atrophy the same as dementia?
No. Brain atrophy is a structural finding, while dementia is a clinical syndrome involving cognitive decline severe enough to affect daily life. A person can have some atrophy without dementia, and dementia evaluation depends on symptoms and function, not imaging alone.
Does brain atrophy always mean Alzheimer’s disease?
No. Alzheimer’s is one cause, but stroke, vascular disease, head trauma, infection, alcohol-related injury, autoimmune disease, and other neurologic conditions can also lead to atrophy.
Can young people get brain atrophy?
Yes. Although it is more often discussed in older adults, younger people can develop brain atrophy from genetic conditions, multiple sclerosis, traumatic brain injury, infections, autoimmune disease, or other serious neurologic disorders.
Does brain atrophy cause pain?
The shrinkage itself is not usually described as painful, but the underlying disease or related complications may cause other symptoms, depending on the cause.
Can lifestyle changes help?
They may help support brain health and lower risk related to vascular and cognitive decline. Exercise, not smoking, healthy diet, sleep, and management of blood pressure, blood sugar, and cholesterol are all supported by major public health guidance.
Final Thoughts
Brain atrophy is a meaningful medical finding, but it is not one-size-fits-all. The real question is what is causing it, how fast it is changing, and whether it is affecting function. In some people it reflects relatively mild age-related change. In others, it may signal a progressive neurologic disease, vascular damage, prior trauma, or another condition that deserves close attention.
The best next step is not to panic over the wording on a scan report, but to connect the imaging with symptoms, medical history, and a full clinical evaluation. Earlier assessment can open the door to treatment of reversible causes, better symptom management, safer planning, and healthier long-term support.